
Cerebral malaria is a serious brain complication of a malaria infection, usually caused by the Plasmodium falciparum parasite. It does not just cause fever and body aches; it can quickly affect the brain, making it a medical emergency, especially in children.
Unlike “ordinary” malaria, cerebral malaria often develops after a child or adult has already had a few days of fever, then suddenly becomes very unwell, sleepy, or has seizures. The good news is that early treatment can save lives, and many people can recover, especially if they get help within hours.
Do you live in or wish to travel to malaria‑prone areas? Have you heard of “cerebral malaria” and want to know what it is, how serious it is, when fever becomes an emergency, and when to seek urgent help? This article is for you.
What Is Cerebral Malaria?
Cerebral malaria happens when malaria parasites infect the body, travel to the brain, and damage the brain’s blood vessels and tissues. It is not just “bad malaria”; it is a brain‑related crisis that can cause coma, seizures, and long‑term problems if not treated fast.
Key points to know:
- It is caused mostly by one type of malaria parasite (Plasmodium falciparum).
- It usually affects children under 5 and people who have not had much malaria before (non‑immune individuals).
- It is most common in areas where malaria‑carrying mosquitoes are common, including parts of sub‑Saharan Africa, Asia, and parts of South America, but it can occur anywhere malaria is present.
How Does Cerebral Malaria Happen?
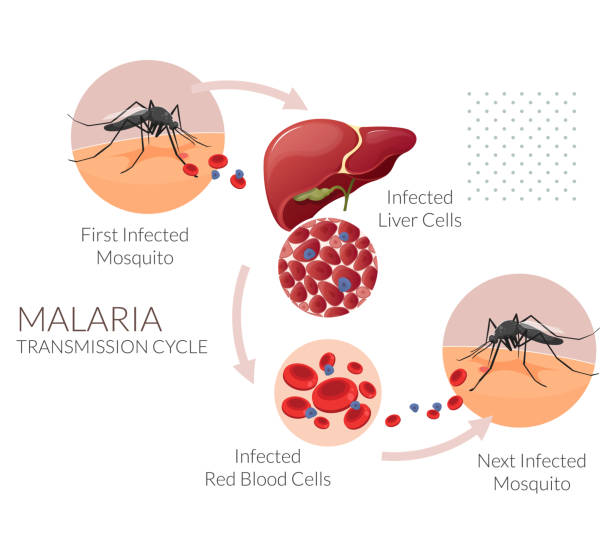
Malaria starts when a mosquito bite puts malaria parasites into the human body.
Here are the steps:
- The parasites first travel to the liver, where they grow for a few days.
- Then they enter the bloodstream and start infecting red blood cells.
- Every 2 – 3 days, the infected blood cells burst, releasing more parasites and causing fever, chills, headaches, and body aches in cycles.
Cerebral malaria happens when:
- Infected red blood cells stick to the inner walls of tiny blood vessels in the brain, blocking blood flow.
- This reduces oxygen and nutrients to brain tissue, causes inflammation and swelling, and can lead to coma, seizures, and, in some cases, death if not treated quickly.
It is not usually caused by a simple “rupture of the blood‑brain barrier with major haemorrhage,” as sometimes oversimplified; it is mainly about blocked blood flow and inflammation in the brain.
Who Is Most at Risk?
Children under 5 and pregnant women are at higher risk of severe malaria, including cerebral malaria, because their immune systems have not had much exposure to the parasite before.
Other risk factors include:
- Living in or travelling to malaria‑endemic areas without good protection.
- Delayed or no treatment for malaria once symptoms appear.
- Nutritional problems or other illnesses that weaken the body.
Although cerebral malaria can affect adults, it is especially dangerous in young children, who may not be able to clearly say what is wrong.
Symptoms of Cerebral Malaria in Children

At first, a child with cerebral malaria may just seem to have regular malaria symptoms: high fever, shivering, headache, and body aches. After a few days, the child suddenly becomes much worse.
Watch for these danger signs (if any of these appear, seek urgent medical help):
- High fever that does not improve with usual treatment.
- Very sleepy, confused, or hard to wake up.
- Seizures or fits (jerking arms and legs, staring spells, or unresponsiveness).
- Repeated vomiting or not being able to drink or eat.
- Fast or difficult breathing, unusual breathing patterns, or grunting.
- Stiff neck or severe headache (possible sign of brain swelling or another infection).
- Unusual eye movements, crossed eyes, or one side of the body weaker than the other.
In older children or adults, symptoms may also include:
- Sudden confusion or strange behaviour.
- Difficulty speaking or understanding.
- Severe dizziness or balance problems.
When is Cerebral Malaria an Emergency
Cerebral malaria can be life‑threatening within hours. Any child with a fever plus one or more of the following must be taken to the nearest clinic or hospital immediately:
- Unable to stay awake or answer questions.
- Having seizures or fits.
- Breathing rapidly, noisily, or with difficulty.
- Extremely sleepy or “not acting like themselves.”
- Repeated vomiting or cannot drink fluids.
Delaying treatment greatly increases the risk of death or long‑term brain problems.
How Is Cerebral Malaria Diagnosed?
Doctors usually diagnose cerebral malaria in two steps:
- Confirm malaria infection: Using a malaria blood test (microscopy or rapid test) to check for malaria parasites.
- Check for brain involvement and other causes by looking at symptoms like coma, seizures, or abnormal behaviour. In some hospitals, they may do blood tests, lumbar puncture (spinal tap), or brain imaging (CT/MRI) to rule out meningitis, encephalitis, or other brain problems.
In areas with limited resources, doctors often rely on the child’s symptoms plus the malaria test result and may start treatment before advanced tests are available.
Cerebral Malaria Treatment and What Happens Afterwards
If cerebral malaria is suspected, treatment must start as soon as possible.
- Antimalarial drugs are given by injection or drip (not just tablets) in a hospital, usually for several days.
- The child may also receive fluids, medicines for seizures, treatment for low blood sugar, anemia, or other complications, and close monitoring.
Outcomes:
- With early and correct treatment, many children recover fully.
- Some children may have long‑term problems, such as:
- Repeated seizures (epilepsy).
- Speech or learning difficulties.
- Weakness on one side of the body or balance problems.
Not every child has severe problems, and rehabilitation support (like physiotherapy and speech therapy) can help improve recovery over time.
Prevention of Malaria and Cerebral Malaria

Prevention is the best way to stop cerebral malaria from happening. Key steps:
- Sleep under insecticide‑treated bed nets, especially long‑lasting nets that keep working for up to 3 years.
- Use mosquito repellent, window screens, and protective clothing in areas where mosquitoes are common.
- Follow local health‑clinic advice: Pregnant women may be given preventive medicines (such as sulfadoxine‑pyrimethamine) at regular antenatal visits. Children in some areas may receive seasonal or targeted preventive treatment to reduce severe malaria risk.
No prevention method is 100% effective, so:
- Always treat fever quickly with medical care.
- Do not ignore a child’s fever just because they are using a bed net or taking preventive drugs.
Other Illnesses That Can Look Like Cerebral Malaria
Some other diseases can also cause fever, confusion, or seizures, so doctors must check carefully. They include:
- Meningitis or encephalitis: Severe headache, stiff neck, a very sleepy child, may have a rash.
- Typhoid fever: Fever with stomach pain, vomiting, or diarrhoea.
- Dengue fever: Fever, rash, and sometimes bleeding or low platelets.
- Other infections or brain problems that need different treatment.
This is why it is important for a child with fever and worrying signs to be seen by a doctor rather than self‑treated at home.
Physiotherapy and Recovery After Cerebral Malaria
If a child survives cerebral malaria but is left with:
- Weakness on one side,
- Trouble walking or balancing,
- Difficulty with speech or fine movements, they may benefit from physiotherapy and other therapies.
Physiotherapy can help:
- Improve strength, balance, and walking.
- Support better posture and movement.
- Work with families to continue simple exercises at home.
Recovery takes time, and not every child recovers completely, but early and consistent therapy can make a big difference in how well a child functions.
FAQs
No. Regular malaria causes fever, chills, and body aches. Cerebral malaria is a severe brain complication that can cause coma, seizures, or long‑term problems if not treated quickly.
Yes, many children recover fully, especially if they receive early treatment in the hospital. However, some children may have lasting problems such as seizures, learning difficulties, or movement issues.
To prevent malaria in children, use insecticide‑treated bed nets, seek medical care as soon as the fever starts, and follow local prevention advice (for example, preventive medicines in some areas).
Go immediately if the child is very sleepy, confused, or hard to wake; has seizures or fits; is breathing fast or with difficulty; keeps vomiting or cannot drink.
- Idro, R., & Newton, C. R. (2010). Cerebral malaria: Mechanisms of brain injury and implications for future research. Pediatric Research, 68(5), 360–367. https://doi.org/10.1203/PDR.0b013e3181f4b3b8
- Guenther, G., et al. (2021). Pediatric cerebral malaria. Pediatric Critical Care Medicine, 22(1), e1–e10. https://doi.org/10.1097/PCC.0000000000002523
- Song, X., & colleagues. (2022). Cerebral malaria induced by Plasmodium falciparum: Mechanisms and outcomes. Frontiers in Cellular and Infection Microbiology, 12, 939532. https://doi.org/10.3389/fcimb.2022.939532
- Taylor, T. E., et al. (2015). The pathogenesis of pediatric cerebral malaria. Blood, 125(14), 2167–2175. https://doi.org/10.1182/blood-2014-10-606901
- Postels, D. G., & Boivin, M. J. (2025). Cerebral malaria. Current Opinion in Pediatrics, 37(2), 181–188. https://doi.org/10.1097/MOP.0000000000001345
- WHO. (2023). Guidelines for the treatment of malaria (4th ed.). World Health Organization. https://www.who.int/publications/i/item/9789240076121
- Ibrahim, O. R., et al. (2024). Clinical and laboratory predictors of poor outcomes in cerebral malaria. Oman Medical Journal, 39(3), e640. https://doi.org/10.5001/omj.2024.39.03.08
