
What is Jaundice?
Jaundice is a clinical sign of a condition that causes yellowing of the skin, whites of the eyes, and lips. It occurs when there is excess unconjugated or even conjugated bilirubin in the blood.
The whites of the eyes can get a little less white with age or from lack of sleep, but in jaundice cases, they are “abnormally yellow”. Some patients report that it isn’t just that their skin and eyes look yellow; it’s that they hurt so badly, and the “glowing” can be a bit embarrassing. However, jaundice itself is not painful, but the underlying condition that causes it may lead to pain or discomfort.
In the newborn, jaundice is quite common and can be harmless if physiological. But, pathological jaundice requires immediate care.
Jaundice is usually noticed as yellowing of the skin and eyes, before it is confirmed by a liver function test that shows your total bilirubin level. In jaundiced patients, their bilirubin levels are higher. In some cases, your GP may order extra tests, blood works and scans, depending on the nature of your condition.
Pathophysiology of Jaundice
How does jaundice happen?
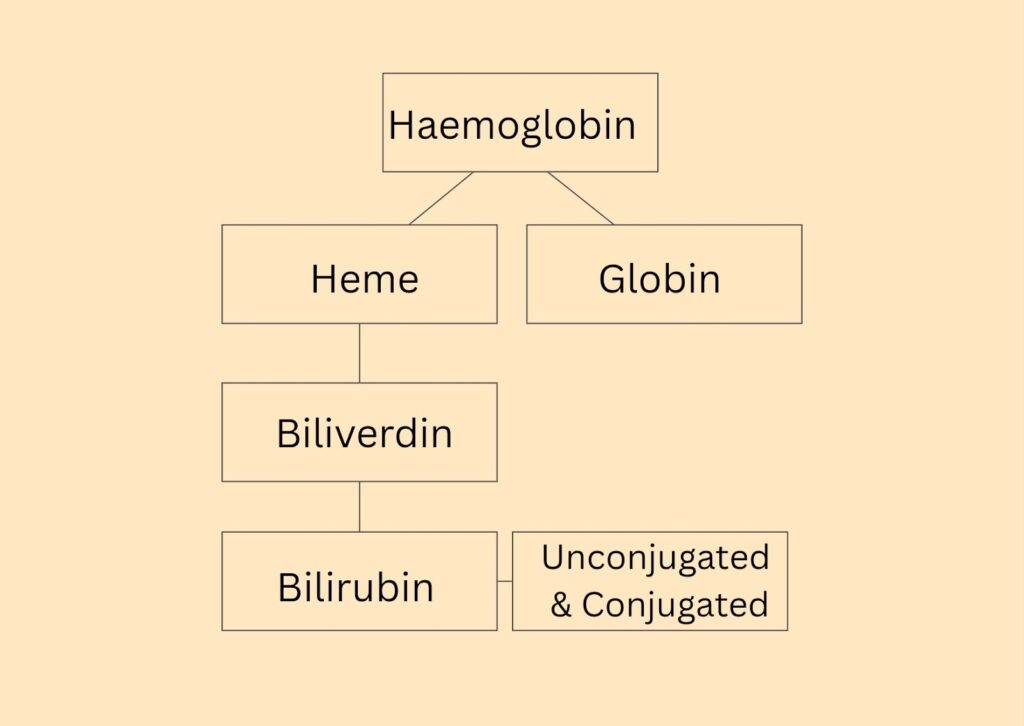
When red blood cells complete their 120-day lifecycle, it breaks down, releasing haemoglobin. This haemoglobin is the protein component and oxygen-carrying component of the blood.
Red blood cells are broken down in the spleen, liver, and bone marrow before they are taken to the liver for processing.
Haemoglobin splits into heme and globin. The globin is recycled while the heme further breaks down to biliverdin. Biliverdin is first converted to unconjugated bilirubin, which is toxic and fat-soluble.
The unconjugated bilirubin binds to albumin and is transported to the liver, where it is converted to conjugated bilirubin and excreted in the bile, processed in the intestines, and disposed of in the stool and to a small extent, in urine.
In the gut, bilirubin is converted to urobilinogen and oxidized to stercobilin, which is responsible for the yellow coloration of the faeces. A small portion of the urobilinogen goes to the kidneys and is oxidized to urobilin, which gives urine its yellow color.
Now, when there is a problem with the hepatobiliary circulation (the blood flow between the liver and the gallbladder or other organs), bilirubin may be deposited or recirculated into the blood.
And when it recirculates, that colouring, which you would expect in the faeces, will now colour the skin and the whites of the eye.
Therefore, conditions that increase haemoglobin levels and unconjugated and conjugated bilirubin will likely cause jaundice. Also, conditions that impair the excretion of any form of bilirubin increase the risk of jaundice.
The liver enzyme (UGT1A1) conjugates bilirubin so it can be excreted. But in neonates, UGT1A1 activity is low, especially in preterm infants. Hence, more unconjugated bilirubin roams freely and is reabsorbed into the blood, causing jaundice.
Neonates also have an immature gut and increased enterohepatic circulation, further allowing more unconjugated bilirubin to be reabsorbed.
Causes of Jaundice
There is neonatal jaundice and adult jaundice; the causes are different in both situations.
Neonatal Jaundice

- Physiological jaundice of the neonate:
This is neonatal jaundice that occurs in the first week after birth. Normally, after a child is born, they are very delicate, and some of their organs are not well developed.
Now, as red blood cells complete their life cycle and begin to break down, their byproducts (bilirubin) may conjugate immaturely, overwhelm the liver, or be recycled back into the circulation too quickly.
This leads to the deposition of that bilirubin in the skin, the whites of the eye, and the lips.
Physiologic jaundice appears after 24 hours, peaks between days 3 and 5 in babies carried to full term, and then resolves. It is sometimes considered a normal, self-limiting process because it resolves on its own within 1 to 2 weeks as the liver matures and the processed bilirubin is cleared.
Jaundice that happens less than 24 hours after birth (whether conjugated or unconjugated) is considered pathological and requires prompt workup.
- Breastfeeding jaundice in the neonates:
If the child is not fed enough breast milk, they will, by extension, not receive the nutrients and hydration needed for proper organ development. To supplement the nutrients that the body needs, the intestines reabsorb more bilirubin than they should. Overall, this suboptimal milk intake increases bilirubin levels.
Surprisingly, breastfeeding jaundice is more common in breastfed babies than in formula-fed babies. It can also occur if the child is given water or any other substance apart from breast milk or its substitutes.
- Breast milk jaundice:
This mirrors physiological jaundice because, in this case, the child is well fed, yet their liver is not fully developed to conjugate the bilirubin and dispose of it properly.
The difference between physiologic jaundice and breast milk jaundice is that the latter develops after the first 4-7 days of life, while the former commonly happens in the first week of life. Also, physiologic jaundice resolves faster than breast milk jaundice. On similarities, both physiologic jaundice and breast milk jaundice can be caused by unconjugated (indirect) hyperbilirubinemia.
In some cases of breast milk jaundice, the cause is not known.
- Hemolytic/pathological jaundice in children
Can be due to blood-group incompatibility (ABO/Rh), G6PD deficiency, sepsis, large cephalohematoma (skull bleed from birth trauma), prematurity, or congenital liver/biliary disease. These often cause unconjugated jaundice in children, because the rapid breakdown of red blood cells produces more heme than the liver can conjugate.
Adult Jaundice

Jaundice that occurs in adults is pathological and can be caused by diseases of the liver, gallbladder, or pancreas.
Jaundice in an adult can result from:
- Liver cirrhosis: Which occurs with excessive intake of alcohol.
- A damaged gall bladder
- Non-alcoholic fatty liver disease or alcoholic fatty liver disease. Jaundice is not common in fatty liver disease. However, the liver can become scarred in fatty liver disease, which can turn into cirrhosis and cause jaundice.
- Hepatomegaly
- Cholecystitis
- Benign liver lesions like intrahepatic simple cysts can only cause jaundice if they obstruct bile flow
- Pancreatic conditions, e.g., Pancreatitis
- Mononucleosis: Mono can mess with the liver, causing jaundice symptoms
Risk Factors of Jaundice
The following groups of people have an increased risk of having jaundice:
- Neonatal factors:
- A baby born premature leading to an immature liver and higher bilirubin production.
- Poor feeding/dehydration when breastfeeding is inadequate.
- Family history or a previous sibling with significant neonatal jaundice or kernicterus.
- Birth trauma/extensive bruising. The bleeding & bruising increases bilirubin load.
- Hemolytic factors:
- People with hemolysis from ABO/Rh incompatibility, G6PD deficiency, or other red-cell disorders.
- Liver-related factors:
- Drug-induced hepatic damage occurs when the liver is damaged from misusing or abusing drugs, and yes, including the abuse of legal or prescribed medications.
- Excessive alcohol intake damages the liver and predisposes patients to liver cirrhosis and jaundice.
- Infectious factors:
- Infection, metabolic or endocrine disease, such as sepsis, hypothyroidism, or inborn errors of metabolism.
- Ethnicity & maternal factors:
- Some populations (e.g., East Asian) and maternal diabetes/polycythemia raise risk.
Types of Jaundice
Jaundice can also be classified into direct and indirect jaundice.
- In direct jaundice, there is excess deposition of conjugated bilirubin in the skin, the whites of the eye, and the lips.
- In indirect jaundice, there is excess deposition of unconjugated bilirubin. Most neonatal cases are unconjugated.
Clinically, jaundice is also classified as prehepatic, hepatic, or posthepatic based on where the problem occurs.
Symptoms – Clinical Features of Jaundice

- Yellowing of the whites of the eyes (scleral icterus)
- Yellowing of the skin, which usually starts on the face/head and spreads downward as the bilirubin level rises.
- Pale stool color
- Yellow or dark urine even after drinking significant amounts of water
- Poor feeding, poor weight gain, sleepiness, irritability, or muscle wasting.
- High-pitched cry, hypotonia, lethargy, seizures (suggest bilirubin encephalopathy). These are all signs of severe toxicity.
- Fatigue or malaise
- Abdominal distension with liquid (Ascites) seen in liver failure.
NB: A very rapid rise in yellowing (e.g., onset <24 hours) or persistent jaundice beyond 2 weeks is a red flag, and you should escalate the patient’s care.
Diagnosis of Jaundice
- Liver function tests (LFTs): A liver function test shows total bilirubin levels (direct and indirect). Direct refers to the amount of conjugated bilirubin in the blood, while indirect is for the unconjugated bilirubin fractions.
- Urine analysis: Bilirubin appears in urine only in conjugated jaundice. If it is high, then the levels in the body and blood will also be high.
- CBC/reticulocyte count: Complete Blood Count (CBC) shows the haemoglobin levels. Hemolysis in jaundice lowers the Hb count and raises reticulocytes, causing anemia.
- Blood tests: CRP levels and blood cultures can be done if infection or sepsis is suspected.
- Scans: Elevated direct bilirubin levels are common with liver disease, cholestasis, and cholecystitis. If these conditions are suspected, they can be confirmed with an ultrasound/HIDA.
- Others: Blood group and direct Coombs tests, G6PD tests, peripheral smear, thyroid tests, and metabolic screen, where suspected.
Differential Diagnosis
These are conditions that look like jaundice but are not jaundice:
- Hemolytic Disease (ABO/Rh Incompatibility): An immune condition where maternal antibodies destroy newborn red cells, causing a fast rise in bilirubin. It presents within 24 hours, with a positive direct Coombs test and high reticulocyte count.
- G6PD Deficiency: An inherited enzyme defect that causes episodes of red-cell breakdown after oxidant exposure, producing high bilirubin. The differentiating clues here are a history of trigger exposure, intermittent hemolysis, and a low G6PD assay.
- Biliary Atresia: Progressive blockage or absence of extrahepatic bile ducts in infants, causing conjugated jaundice. It can be suspected with pale stools, dark urine, and abnormal liver tests that persist beyond the neonatal period.
- Neonatal Sepsis: A blood infection in the newborn that can impair liver function and raise bilirubin levels. To differentiate this, look for fever or low temperature, lethargy, raised inflammatory markers, and positive blood cultures.
- Congenital hypothyroidism: Low thyroid hormone from birth that slows bilirubin metabolism and gut motility. Think of this when jaundice is prolonged with poor feeding, low muscle tone, and abnormal thyroid tests (high TSH, low T4).
- Cephalohematoma/Extensive birth bruising: Localized bleeding under the scalp or large bruises that raise bilirubin as the blood is reabsorbed. Differentiate by visible scalp swelling and a history of traumatic delivery.
Complications of Jaundice
Jaundice does not only come with the “Yellow coloration.” It sometimes comes with irreversible brain injury (acute bilirubin encephalopathy/kernicterus), causing:
- Seizures
- Eye movement problems
- Hearing loss
- Delayed developmental milestones in neonates
- Long-term motor disorders
- Cognitive delay
To prevent these complications, jaundice must be recognized and treated early.
Jaundice Treatment

- Phototherapy:
This is the first line of treatment for unconjugated jaundice. Phototherapy is mainly used in neonates and is rarely required in adults. In traditional settings, jaundiced babies are taken outside to receive the morning sun. However, controlled medical phototherapy is preferred over sunlight exposure.
In a modern medical setting, the individual is placed in a phototherapy booth that emits a blue light. This light processes the bilirubin deposited in the skin, aiding its excretion through the urine or faeces.
- Exchange transfusion:
In severe cases, cases where the bilirubin is rapidly rising, and some hemolytic cases, there is a risk of neurotoxicity. This treatment helps to normalize the thresholds.
- Treating the underlying cause:
If the cause is hemolysis (ABO/Rh, G6PD), the patient is treated with specific therapy (e.g., IVIG for immune hemolysis); if infection, they are started on antibiotics.
- Supportive measures:
Ensure adequate feeding and hydration (breastfeeding support or supplementation when needed). This helps with bilirubin clearance.
What Does Physiotherapy Have to Do with Jaundice?
Physiotherapists do not treat jaundice, but its complications. Because of these complications, you may be referred to a physiotherapist.
Severe cases of jaundice can cause bilirubin encephalopathy or irreversible brain injury. In this case, the physiotherapist plays a longer-term rehabilitation role alongside the neurodevelopment team. They help in motor retraining of delayed or lost milestones and functional recovery.
For adults, fatigue and malaise can lead to functional impairments. And the patient may need physical therapy to rebuild strength and regain functional activities of daily living, too.
Jaundice may require a multidisciplinary team effort, depending on the extent of the condition and the complications that have resulted.
Warning Signs for Physiotherapy
Your PT may have to treat with caution or stop routine therapy and refer urgently to the neonatal medical team if they see any of these:
- If the child or individual is still yellow at the time of referral
- Rapid increase in visible jaundice or persistent jaundice beyond 2 weeks
- In cases where seizures occur after or during the jaundice
- If the patient is unstable, worsening, lethargic, or their responsiveness decreases
- Sudden abnormal tone: hypotonia or hypertonia
Conclusion
Jaundice starts small. A yellow tint on the eyes and soon, it spreads to the skin. But that small sign can tell a big story about the liver, blood, or bile flow. In neonates, settle with careful feeding, monitoring, and the right treatment. The important lesson is to know the warning signs and act early rather than wait.
In adults, a little bit of yellowing on the whites of the eyes is no cause for concern. But if you take alcohol frequently, have liver disease, or have a family member who has/had one, you should definitely go get checked out.
With prompt testing and timely treatment, most people recover fully. And when complications occur, early rehabilitation and follow-up make a measurable difference. If you notice fast-spreading yellowing, poor feeding, extreme sleepiness, or pale stools, seek medical care as soon as possible.
- Al-Bedaywi, R. R. R. (2024). Glucose-6-phosphate dehydrogenase deficiency and neonatal hyperbilirubinemia. Journal Article. https://www.nature.com/articles/s41372-024-01927-1
- Ansong-Assoku, B. (2024). Neonatal jaundice. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK532930/
- Bratton, S. (2023). Breast milk jaundice. PubMed. https://pubmed.ncbi.nlm.nih.gov/30726019/
- Cleveland Clinic. (2022, January 17). Jaundice in newborns. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/22263-jaundice-in-newborns
- Cnossen, M. C., et al. (2024). Home phototherapy for neonatal hyperbilirubinemia. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454146/
- Kemper, A. R., et al. (2022). Clinical practice guideline revision: Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics, 150(3), e2022058859. https://doi.org/10.1542/peds.2022-058859
- Lee, H. Y., et al. (2022). Glucose-6-phosphate dehydrogenase deficiency and neonatal jaundice. [Review]. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9170901/
- MedlinePlus. (2025, January 1). Newborn jaundice. U.S. National Library of Medicine. https://medlineplus.gov/ency/article/001559.htm
- World Health Organization. (n.d.). Newborn — management of neonatal jaundice / related recommendations. https://www.who.int/teams/maternal-newborn-child-adolescent-health-and-ageing/handbooks/programme-manager-s-handbook-mncah/recommendations-on-interventions-along-life-course/newborn
